

Dystocia, by Greek root definition, means difficult birth. For the bovine practitioner, it is one of the more frequent emergency call outs. To give some context, internationally reported dystocia incidence (in primiparous and multiparous cows combined) varies from 1.5% in Norway to over 13% in the US, with the UK somewhere between those extremes (Mee, 2008). However, this figure can be complicated by the subjective nature of the definition of dystocia.
This article aims to explore the risk factors, causes, approaches and outcomes of dystocia in cattle.
Short-term risk factors
For the sake of this article, short-term risk factors of dystocia are those that occur from the point of conception. The author will discuss these chronologically, starting with the breeding of the dam.
When making breeding decisions, it must be remembered the biggest risk factor for dystocia is calf birthweight. It accounts for 50% of the phenotypic variance, with an increase in the risk of dystocia by 13% for every additional kilogram of birthweight (Johanson and Berger, 2003).
Because of this, sire selection is important for managing the risk of dystocia (Bellows et al, 1971; Gregory et al, 1991; Johanson and Berger, 2003; Berry et al, 2007). Traditionally, sires have been selected for calving ease using Estimated Breeding Values (EBVs) or Predicted Transmitting Ability (PTAs). For dystocia, ‘calving ease direct’ is the value used, with calving ease being negatively correlated with birth weight and gestation length.
Similarly, calf sex is an important contributing factor to calf birthweight, with the odds of dystocia being 25% greater with a male calf than with a female (Johanson and Berger, 2003). The increasing availability of sexed semen has given control over calf sex to the producer, and hence its implications on dystocia risk should be considered at breeding.
Lastly, in cases of embryo transfer, pregnancies from both in vivo and in vitro embryos have been shown to carry a higher risk of dystocia than those of artificial insemination (Zaborski et al, 2009).
After the dam has been bred, a risk factor that would present next, at the point of pregnancy diagnosis, is the number of fetuses carried by the dam. Twin pregnancies are more likely to encounter dystocia than single pregnancies, and an economic analysis has suggested that manual reduction of one of the twins is the most economically advantageous practice on their detection (Zaborski et al, 2009; Cabrera and Fricke, 2021; Morek-Kopeć et al, 2024).
After breeding decisions have been made, nutrition of the dam is the main remaining short-term risk factor for dystocia. Proper feeding during pregnancy is particularly important in heifers, as body weight of the dam is negatively correlated with the probability of dystocia in both dairy and beef breeds (Schröder and Staufenbiel, 2006; Zaborski et al, 2009). Cows fed on a high-energy diet over the whole lactation have been shown to have more prolonged parturition and greater rates of dystocia (Maree, 1986). The evidence on whether body condition score in the dry period impacts on dystocia is mixed (Zaborski et al, 2009; Rodriguez et al, 2021). Restricted feeding of the dam does not significantly affect calf birthweight, owing to supplementing of calf growth with energy from body reserves, and severe restriction may lead to greater risk of dystocia (Hickson et al, 2006; Mee, 2008). The mineral status of the dam also plays a role in the risk of dystocia (Hidiroglou, 1979; Bahrami-Yekdangi et al, 2022; Vieira-Neto et al, 2024).
Long-term risk factors: pre-conception
While short-term management issues are the focus in herd ‘outbreaks’ of dystocia, herds with ongoing issues should address long-term risk factors. The following factors have been identified in the literature and are available to be addressed:
Bull selection
As mentioned previous, traditionally bulls have been selected for calving ease using EBVs or PTAs. However, different to the ‘calving ease direct’ mentioned previously, ‘calving ease daughters’ is an indicator of how easy calving any female offspring is likely to be and therefore carries a long-term gain.
EBVs are traditionally based on phenotypic data on this animal and its parentage and offspring, relying on accurate recording. The accuracy of EBVs depends on accuracy of recording of its own traits, the number of recorded parents, grandparents or offspring and the heritability of a trait (eg the percentage of variation which is attributed to genetic factors). The heritability of calving ease (direct and maternal) is estimated to be below 0.1. EBV units are those of the trait, for example, kilograms for weight and percentage of unassisted calvings for calving ease. EBV charts typically display a ‘best guess’ and a standard error bar, indicating that there is a 67% chance that the value is within this bar (and therefore a one-in-three risk that it is not). This is especially relevant for young or minority breed bulls where this information has to be used with caution.
While it is obvious that great inaccuracies are inevitable, this has been the ‘best guess’ for many decades, and a strategy could be to select bulls with positive calving ease, with the number and accuracy both being important.
Heifer selection
On the maternal side, pelvic measurement could be a selection criterium pre-breeding, which is well established for beef herds. This can be used in combination with direct calving ease EBVs. However, inter-operative variation has been identified as an issue, therefore, it should be done consistently by the same person, such as using the same veterinarian (Vernooij et al, 2020).
The Agriculture and Horticulture Development Board provide PTAs for calving ease (direct and maternal), while genomic PTAs for stillbirth exist with anecdotally excellent reliability. Stillbirth is easier to record and less subjective than calving ease and therefore a suitable proxy for calving ease. This is an area of ongoing research and evaluation (Fonseca et al, 2022).
Causes
The causes of dystocia in cattle are vast, and the consequence of the risk factors discussed earlier in the article. Causes are easily identified when categorised, and over the years, multiple methods of categorising them have been published.
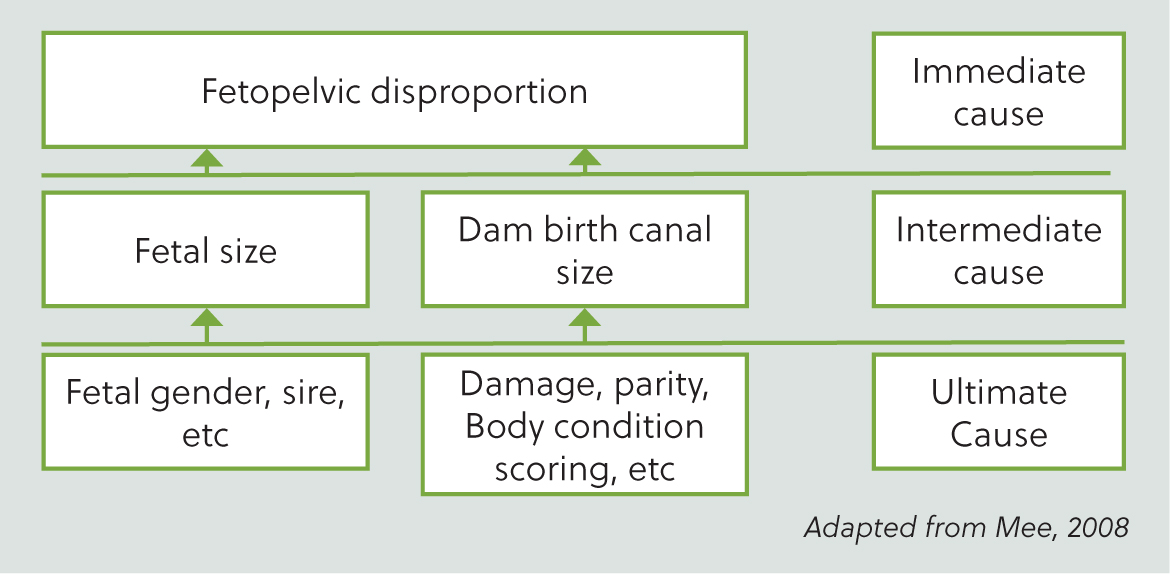
Mee (2008) published a system that displays how a single cause can be multi-layered. In this system, immediate causes (the cause that presents itself at time of parturition) result from intermediate causes (a secondary underlying reason), which in turn result from ultimate causes (a primary underlying reason). Using fetopelvic disproportion as an example, this system is displayed in Figure 1.
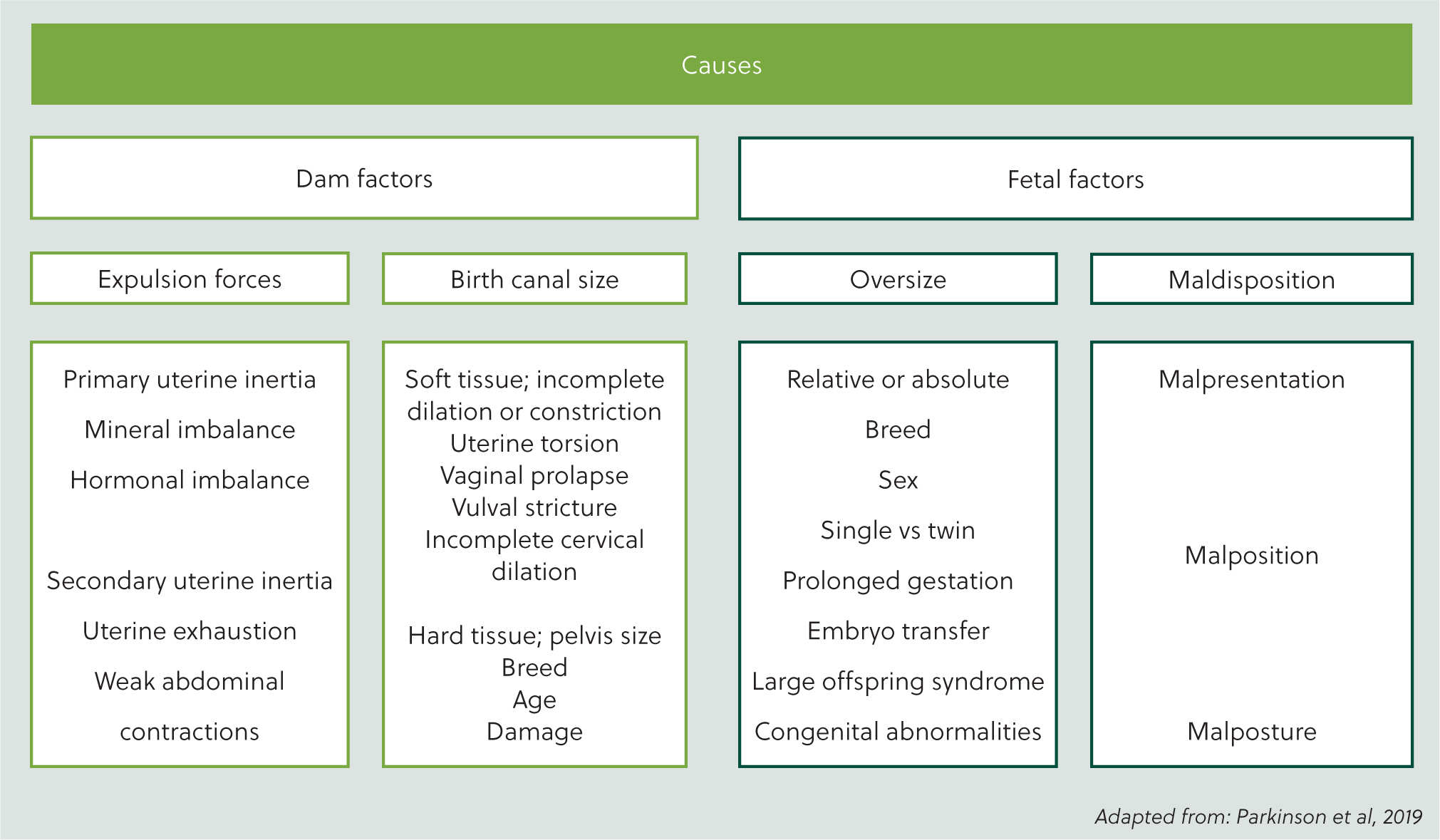
Alternatively, causes of dystocia can be categorised into causes related to the dam, such as uterine torsion, improper cervical dilation or failure of uterine expulsive forces, as well as causes related to the foetus, such as relative or absolute size, deformities, pre-partum death and malposition.
Discussing these individual causes, fetopelvic disproportion is considered one of the major causes of heifer dystocia in both beef and dairy breeds. Outside of just heifers, fetal macrosomia (larger than average foetus) can also cause incompatibility between the dams birth canal and fetal size, and is more prevalent in multiparous cattle (De Amicis et al, 2018). The occurrence of dystocia due to fetal maldiposition is common, and higher in multiparous cattle. Stillbirths, as a cause of dystocia, are reportedly higher in both primiparous and multiparous dairy cattle compared to beef cattle.
Sporadic causes of dystocia include uterine hydrops (hydrallantois and hydramnion). Hydrallantosis makes up around 85–95% of the uterine hydrops cases seen, with a poor prognosis likely for the dam. An increased incidence of hydrallantois has been reported with pregnancies from implanted in-vitro fertilised embryos (House, 2020). Large/abnormal offspring syndrome (LOS/AOS), is predominantly linked with breeding technologies, including in vitro production of embryos, but it rarely occurs naturally (Nava-Trujillo and Rivera, 2023).
Approach
When approaching a dystocia, as per any clinical case, a thorough history should be obtained. This will help the clinician decide if intervention is appropriate. Cornell's most recent guidelines for intervention include (Animal Health Diagnostic Centre, 2024)
If intervention is decided, assessment of the environment and restraint to ensure safe examination is essential. Following this, a brief prioritised physical exam can be performed which would highlight signs of a comorbidity (eg hypocalcaemia), followed by appropriate sanitation allowing for thorough vaginal examination. Upon vaginal examination, the veterinarian will then be presented with one of many different scenarios.
In the cases of suspected fetopelvic disproportion, some will be extreme but most will be subtle making diagnosis more difficult. Because of this, people have sought to find useful indicators that can be applied at the point of exam. These include:
If it is still not clear by this point, Jackson (2004) suggested trial traction carried out with great care and limited force.
Examining for fetal maldisposition needs to be methodical and hence can be helped by using the ‘3-ps’ framework mentioned in Figure 2:
At this stage, identification of twins is essential.
Assessing for the remaining sporadic causes of dystocia, some have characteristic features that are palpable on vaginal exam, eg spiral vaginal folds in a post-cervical uterine torsion. Other causes have less specific features, instead relying on combined history and wider physical exam findings, eg primary uterine inertia as seen with subclinical hypocalcaemia.
Lastly, during this exam, fetal vitality must also be assessed. In human obstetrics, fetal scalp blood lactate is used to measure this. However, due to the limitations of farm practice, veterinarians use fetal reflex responses in cattle instead. These reflexes can be in either the anterior presentation (including interdigital, bulbar or swallowing reflexes) or posterior presentation (including interdigital reflex, anal reflex or pulse of the umbilical cord). As fetal acidosis deepens from physiological to moderate to severe, the fetus becomes less likely to respond to the stimuli, eg anterior interdigital reflex response rate goes from 88% to 65% to 20%. (Held, 1983). The fact that these are not absolute means using multiple is essential.
Once the cause of dystocia and fetal vitality are established, options for correction include:
Simoes and Stilwell (2022) describe a clinical reasoning sequence that can be used to help choose which is appropriate:
Unfortunately describing the details of each of these options is beyond the scope of this article.
Outcomes
Multiple studies have assessed the impact of assisted calvings, both per vagina and caesarean section, on long-term outcomes such as production, future reproduction, and cow and calf survival. Literature on this topic is extensive, but some care must be taken in interpreting and comparing results of different studies, owing to most papers classifying dystocia based on subjective interpretation from farmers.
In dairy cattle, dystocia has profound effects on lactational production. Cows subject to a moderate–hard extraction of the calf produced 510 kg less milk than those which gave birth without assistance, and a lower daily volume of both milk fat and protein than unassisted cattle (Roche et al, 2023). These figures are greater than those from other studies however, a significant impact on average daily yield is reported elsewhere. This includes a decrease in 305-day yield by 135 kg (Atashi et al, 2012) and daily milk production of 1 kg less (Gaafar et al, 2011) in dairy cows that experienced dystocia compared to those that did not.
Other significant impacts of dystocia in dairy cows include a negative effect on future reproductive performance, with decreased conception rates, and subsequently increased days open, services per conception and calving interval in cows (Gaafar et al, 2011). These impact on future milk production and reproductive performance, as well as increased disease including increased rates of retained placenta (Roche et al, 2023).
Cows that experience dystocia increase the risk of being culled and having a shorter productive lifespan than those that give birth unassisted. An effect of dystocia on cull risk in both primiparous and multiparous cows, can be influenced by the sex of the calf. Primiparous cows experiencing dystocia had an increased risk of culling by 2.18 or 1.26 times for those giving birth to a bull or heifer calf, respectively, compared with those that calved without assistance. Multiparous cows had an increased risk of dystocia-linked culling of 2.0 and 1.33 times higher for bull and heifer calves respectively, than those without assistance (Morek-Kopeć et al, 2021).
A caesarean section procedure has a similar impact to dystocia on the dams, and shortens the productive life of a dairy cow, with an increased risk of culling of 1.89 (Strapákov et al, 2023). There is also evidence of hepatocellular damage in dairy cattle subject to caesarean section, which was not found in cattle with unassisted calvings (Hussein and Abd Ellah 2008). In beef animals, a caesarean section may be more commonly performed than in dairy cows, and the outcomes are typically more favourable, with a post-operative mortality rate of 6.2% and successful rebreeding reported in 75% of cases (Hiew et al, 2018).
As well as an impact on the dam, dystocia has also been associated with an increased risk of stillbirth (Lombard et al, 2007; Strapáková et al, 2023), and adverse effects on the health and performance of calves born alive. The odds of a heifer calf developing respiratory disease are increased following dystocia, and the risk of mortality after 24 hours is increased with an increasing dystocia score (Lombard et al, 2007). Calves born following dystocia and a prolonged calving period are also more likely to experience metabolic acidosis immediately postpartum. This leads to an increase in the time to attain sternal recumbency and weakens the suckling response after birth. This has been shown to significantly reduce the total weight gain of these calves in the 2 weeks following birth (Murray et al, 2015). This negative impact on calves is similar in those delivered by caesarean section, with 37.6% of calves delivered dead or dying within 24 hours, and higher for calves with prolonged signs of labour prior to surgery (Hiew et al, 2018).
Conclusions
Dystocias in cattle can be a complex decision-making process for the bovine practitioner. They are the product of multiple risk factors, some of which can be controlled, some of which cannot be, resulting in a range of different causes. To establish the cause, assessment needs to be careful and methodical, with clinical reasoning being essential to help decide what the options for correction include. It must also be remembered that the outcomes of the different methods of correction vary, adding an additional layer of complexity to the decision making process.